

Control of Epidemics and Social Diseases in Soviets
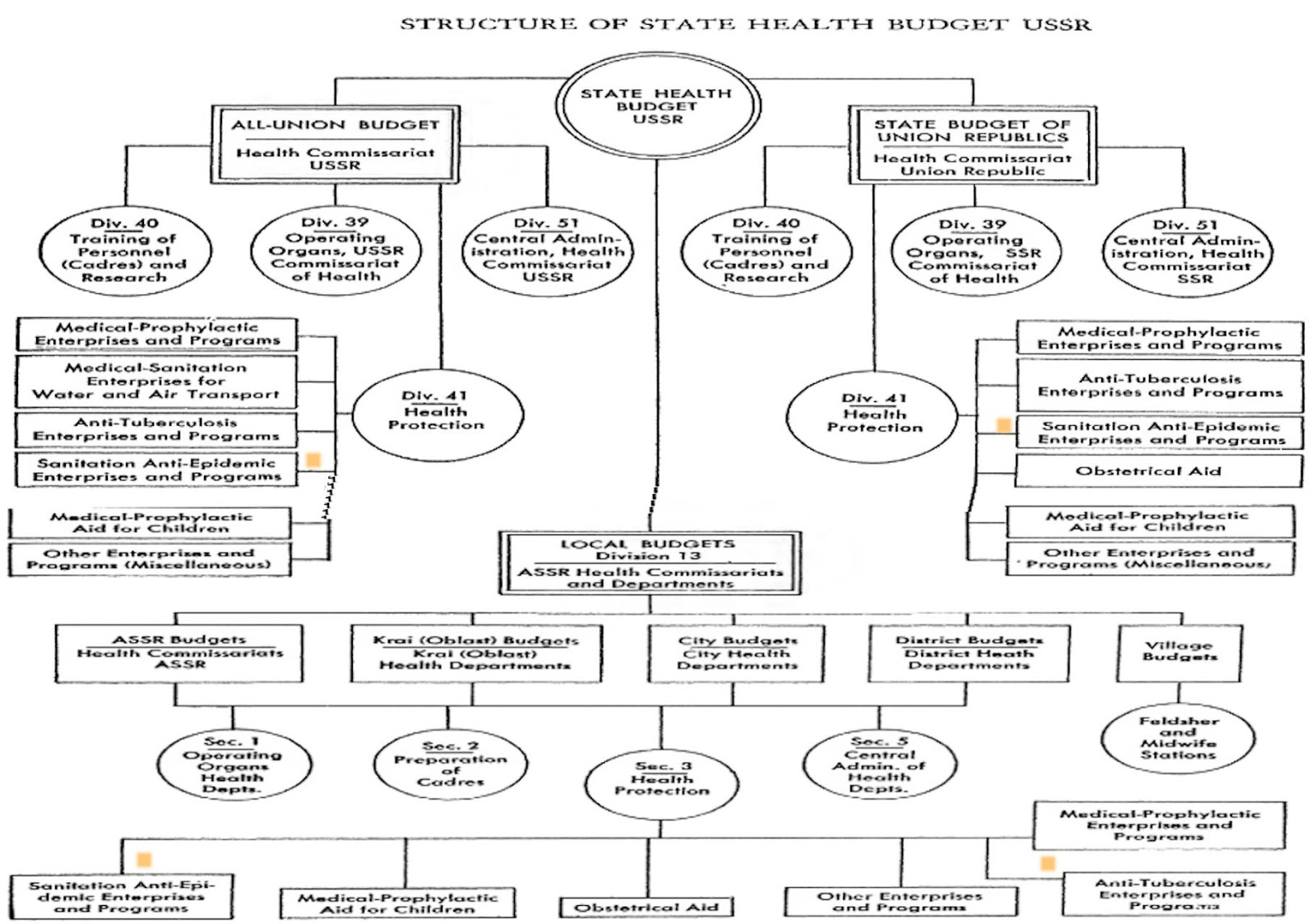 |
| Health Care Budget Structure |
Henry E. Sigerist
(...)
(..)
In the early days of the Revolution, a Medical Division was established by the War-Revolutionary Committee in Petrograd. Upon the personal initiative of Lenin, the Communist Party formulated its health program. The most urgent tasks follow:
1. A determined effort to carry out far-reaching public health measures for the benefit of the
a. Sanitation of living places (protection of soil, water, air)
b. Establishment of communal feeding along principles of scientific hygiene
c. Organization of medicine to prevent the development and spread of contagious diseases
d. Health legislation
2. Combating of social diseases (tuberculosis, venereal diseases, alco holism, etc.)
3. The guarantee of qualified health and medical services available without charge to all.
In February 1918, a Council of Medical Departments was established in Petrograd to coordinate the medical work of the various departments. This measure, however, soon proved insufficient. Epidemics had broken out. Reactionary physicians were neglecting their duty, sabotaging the orders of the new government. White generals were starting the Civil War. The blockading of the country by the Allies was creating a terrific shortage of medical supplies-a barbaric way of fighting a nation. And the enemies of the Soviets found a most powerful ally, small but deadly, when the louse spread typhus throughout the land.
It was soon recognized that in such an emergency nothing could save lives but a central health department invested with full authority to lives but a central health department invested with full authority to control the entire medical service of the country.
On July 11, 1918, the People's Commissariat of Health of the RSFSR was established. For the first time in the history of medicine a central body was directing the entire health work of a nation. The first People's Commissar of Health was Nikolai Alexandrovich Semashko, a close friend of Lenin. Born in 1874, he had led the life of a revolutionary, been arrested and exiled, emigrated in 1907, lived and worked in Geneva and Paris with Lenin, preparing himself for the tasks ahead. He returned to Russia after the February Revolution and was instrumental m the creation of the new Commissariat. He headed it for twelve years.
His task was gigantic. The entire public health service had to be reorganized along new lines. The whole nation had to be mobilized to fight devastating epidemics. The first Workers' Committees to combat these epidemics were created in the cities and larger villages in 1918. Their task was to inspect lodgings and public institutions, to teach the people cleanliness, to distribute soap, to fight the louse. The Communist Party, the trade unions, women's organizations, and youth groups joined in the struggle against disease. It was a fight not only for health but for socialism as well. As Lenin declared in 1919; "Either socialism will defeat the louse, or the louse will defeat socialism."3 Socialism was the victor thanks to the combined efforts of the whole working population under the leadership of the Commissariat of Health.
The work of the first few years was dictated by the emergency. The most urgent matters had to be attacked first. A great deal of improvisation took place. One had to use whatever equipment was available; it was little enough. The medical personnel had to be won over. To the honor of the medical profession, it can be said that in spite of political dissent, the majority of the doctors did not desert the battlefield. They saw that the people were fighting for their very existence.
They dropped their opposition in increasing numbers; medical scientists of world renown offered their services to the government and cooperated loyally with the Commissariat.
Despite the adverse conditions of the early years, the systematically planned work of the Commissariat began on the first day of its existence. The foundations of socialist medicine were laid in the stormy years of Civil War. There was no hesitation in carrying out the program. A network of medical stations was created to provide medical service for mother and child and for the working population in town and country. The sanatoria and health resorts, once used only by the wealthy few, were turned over to the people. A general plan was outlined and it was a mere matter of time-and unceasing hard work, of course-to develop it so that it would fulfill its function.
By 1922 war, famine, and pestilence had been overcome. The young Soviet state had won its first battle. The period of recovery began and health work was carried on under a new slogan: "On from
the struggle against epidemics to the fight for more healthful working and living conditions." Development was naturally slow in the beginning. The country was impoverished; the reconstruction of industry and the electrification of the country, Lenin's great vision, absorbed much of the available energy and money resources. But the policy of Soviet medicine was now clear; the work went on steadily.
The RSFSR Commissariat of Health at first controlled health work in all territory under Soviet jurisdiction. During and after the Civil War, national Soviet republics were created and, on December 30, 1922, the first All-Union Congress of Soviets proclaimed the establishment of the Soviet Union. The constitution, ratified in 1923, created Health Commissariats in all the constituent republics. Decentralization seemed advisable because of the vastness of territory and uneven development of the various regions. The same principles of Soviet medicine were applied in all the republics. The Russian Republic, largest and most important, set the pace and the Commissar of Health of the RSFSR was named Inspector of Sanitation for the Union.
The Constitution of 1923 gave the federal government the right to establish general rules for the protection of health.5 The Constitution of 1936 created a Union-Republic Commissariat of Public Health.
Where the entire health work of a country, preventive and curative, is controlled by a central agency, the work can be planned. This is another characteristic feature of Soviet medicine.
When a five-year plan is being prepared, every health department makes a complete survey of the
conditions in its region. ....
The plans are discussed not only among the specialists, that is the medical workers, but also in the factories and farms, among the working population at large. It is the health of the people that is concerned, and it is obvious that no health plan can be carried out without their active cooperation.
During the First Five-Year Plan, launched in October 1928 and completed in four and one-quarter years, all medical facilities were increased. The health budget jumped from 660.8 million rubles in 1928 to 2,540 million in 1933. But industry came first, particularly heavy industry,
During the First Five-Year Plan, launched in October 1928 and com pleted in four and one-quarter years, all medical facilities were increased. The health budget jumped from 660.8 million rubles in 1928 to 2,540 million in 1933. But industry came first, particularly heavy industry, public health funds. The health budget grew from 2,540 million rubles in 1933 to 9,433 million in 1938. It was 11,960 million in 1941.
The number of physicians in creased from 76,027 in 1932 to 112,405 in 1938. The progress was not only one in quantity but also in quality. Standards were raised throughout the profession.
..epidemics were avoided through a number of integrated measures. One was the practice of limiting epidemic foci by quickly hospitalizing anyone suffering from an infectious disease or suspected of having one. ... Where specialized medical centers were unable to handle a particular problem, the general medical institutions were summoned to their aid.
As a result of this anti-epidemic program, not only did the incidence of many infectious diseases not increase during this dark and difficult period, but some of the diseases even continued their prewar downward trend.
it was due to such precautions as the following: efficient service of medical personnel accompanying troops moving by rail and water; limiting of epidemic foci by enforcing stringent rules on hospitalization; and the fact that from the beginning of the war, all health institutes and hospitals had been converted into a "united instrument for disease prevention."
The tsarist empire was a perpetual playground for epidemics. Small pox, typhus, relapsing fever, typhoid fever and dysentery were endemic diseases in Russia. Cholera and plague visited the population at regu lar intervals. These health conditions were such a constant menace to the West that the rest of Europe looked upon Russia with dread as a permanent source of infection. The government did little to improve conditions. Efforts were made by several associations of physicians, such as the Pirogov Society and the Association of Zemstvo Physicians, but none of them had the power nor the means to apply efficient measures on any large scale. The country was so vast and the population so uneducated that little cooperation could be expected.
Although health conditions were bad enough before 1914, they became infinitely worse during World War l.* The 14 million soldiers who were mobilized and the millions of refugees who fled from the war zones to interior regions of the country created ideal conditions for the spread of epidemic diseases. Health authorities were not idle, but the administrative machinery was so hopelessly slow that it took more than a year before the soldiers could be vaccinated against typhoid and cholera, and more than two years before anti-tetanic vaccination was generally applied.
* L. Tarassevitch, Epidemics m Russia Since 1914. Report to the Health Committee of the League of Nations. Epidemiological Intelligence, No. 2, March 1922, and No. 5, October 1922.
In 1915 an epidemic of typhus broke out at the Turkish front and one of relapsing fever at the Galician front. During the same year, typhus was brought to Samara by Turkish prisoners. Conditions be came worse during the winter of 1916-1917. Armies were exhausted, transportation had broken down in many regions, and supplies were giving out. In the summer of 1917, scurvy was observed on all fronts. During the winter of 1917-1918, there was an outbreak of typhus in Petrograd, but it was overcome after a relatively short time. Then, in the autumn of 1918, prisoners returning from Germany brought influenza with them. It was an unusual instance of an epidemic reaching Russia from the West. Previously, nearly all had come from the East. During the same autumn, there was a new attack of typhus; this time it took a firm hold of the country and spread over a great deal of the territory with devastating effects. The Civil War followed. The popu lation, which was in constant motion, carried diseases everywhere.
The Allied blockade deprived the country of most necessary medical supplies. When the Civil War subsided in 1921, it was followed by the great famine and various epidemics, which made a combined attack upon the hard-hit population. Conditions developed such as the Western world had not seen since the Middle Ages. The Commissariat of Public Health, supported by the Communist Party, medical workers, and large sections of the population, fought a heroic battle. A Central Epidemics Commission under the presidency of Health Commissar Semashko was organized to lead the campaign.
The chief enemy was typhus, a foe well known to the Russians. In the twenty years before the Revolution, there had been an average of 82,447 registered cases annually. Whenever there was a famine or a crop failure, the morbidity more than doubled. During the war, the disease spread slowly but steadily. In 1915, 154,800 cases were registered. The great pandemic started, as we have already noted, toward the end of 1918. It invaded the country from three centers: Petrograd, the Romanian front, and the Volga region. It reached its climax in 1920, declined in 1921, and flared up again in 1922 chiefly in the Volga region, the center of the famine district. After 1923 the incidence of typhus declined steadily. It is very difficult to give accurate figures because the registration of diseases obviously breaks down when a country is completely disorganized. During the Civil War, many cities changed hands six or seven times. Hence the collection of statistical data was almost impossible. The number of registered cases follows: **
** N. Semaschko, "Das Gesundheitswesen in Sowjet-Russland," Deutsche Medizinische Wochenschrzft, 1924, vol. 50, pp. 213-214, 243-244. Appendix VI, based on later, corrected data, gives slightly higher figures for typhus and relapsmg fever in 1922.
Typhus
YEAR NUMBER OF CASES PER 10,000 POPULATION
1918 130,164 21.9
1919 2,119,549 265.3
1920 3,354,656 393.9
1921 633,250 54.0
1922 1,401,145 109.2
Everyone agrees that these figures are much too low. Tarassevitch, a Russian epidemiologist, assumes that during the four years from 1918 to 1922 thirty million cases of typhus occurred. For various epidemic logical reasons discussed by Semashko it is likely that Tarassevitch's estimate is somewhat too high. There can be no doubt, however, that this typhus pandemic was one of the most terrible that the world had ever seen. The mortality amounted to about 10 per cent. It was difficult to fight the disease because of the serious shortage of the two most necessary commodities, soap for cleanliness and fuel for disinfection. People lived in crowded habitations, undernourished, and exhausted by civil war. The authorities did all that was humanly possible in such a great emergency. Two hundred and fifty thousand beds were made available for the treatment of infectius diseases. The railroad lines were watched and numerous quarantine stations were established at im portant railroad junctions. Passengers were taken from trains, were bathed and disinfected, and sick persons were isolated. Propaganda was earned on by means of pamphlets, posters, lectures and exhibitions; special exhibits mounted in railroad cars were sent throughout the infected areas to enlighten the populat10n. Entire sections of a town were cleaned and disinfected during special "bath weeks." But it was an uneven fight, and the pandemic declined only after sufficient immumzation had been built up. Throughout the 1920's, typhus continued to be a serious problem. Although there was a steady decrease in morbidity, 29,417 cases, or two for every 10,000 population, were registered as late as 1929.
Even as late as 1937, there were regions where general conditions were such that an epidemic of typhus could have easily developed. Eradication of the disease was made a major objective of the Third Five-Year Plan, and by 1940 it had been reduced to a few scattered cases in these regions. Testifying to the success of the anti-typhus effort is the fact that although conditions favorable to the disease existed in some of the evacuation areas from late 1941 through 1943, it was never permitted to spread. The Herculean efforts of the various health authorities and community groups rapidly controlled local outbreaks. A new vaccine was available for large-scale use in the affected areas in 1942. These inoculations are reported to have met their purpose of providing specific immunity against typhus, and the award of the coveted Stalin Prize to the
two scientists who developed the vaccine testifies to its significance.
Relapsing fever is a close companion of typhus. It is transmitted by lice, like typhus, but is less deadly. The mortality is from two to three per cent. Like typhus, it was endemic in Russia; from 1887 to 1911 the average number of cases annually amounted to 31,720.53 The morbidity increased during the first world war, and from 1918 to 1922 relapsing fever followed the course of typhus very closely. The official figures are the following:
Relapsing Fever
YEAR NUMBER OF CASES PER I0,000 POP
1918 16,661 2.8
1919 251,3 42·3
1920 1,453,424 127-3
1921 763,131 65.1
1922 1,446,722 112.7
The treatment of relapsing fever is relatively easy, since the disease 1s caused by a spirochaeta which can be destroyed through injections of salvarsan or similar preparations. As a result of the blockade, however, salvarsan was not available in sufficient quantities during the time of the pandemic. Like typhus, relapsing fever decreased after 1923. Inci dence dropped from 19.3 per 10,000 in 1923 to 3.8 m 1924 and continued to drop rapidly thereafter. Cases continued to develop for several more years, but once salvarsan became available in sufficient quantities relapsing fever ceased to be a serious menace. It now ranks among diseases which are practically non-existent in the Soviet Union.
Plague was once one of Russia's most dreaded diseases; history reports many epidemics of it that ravaged the country and destroyed millions of human lives.5 ;; In western Europe it has practically disappeared since the seventeenth century, but in tsarist Russia cases developed nearly every year. From 1905 to 1914, 3,500 deaths from plague were reported. It was very fortunate that no general epidemic broke out between 1918 and 1922; otherwise the Russian population might have been largely destroyed. There was a serious epidemic in Manchuria from 1920 to 1921, and a number of cases occurred in the Far Eastern section of the Soviet Union. Fortunately, these latter could be isolated and the epidemic did not spread.
Russia had several foci of plague: one in the North Caucasus, another in the Kirgiz steppes north of the Caspian Sea, and a third in Mongolia. Until recently, a few cases of plague were reported every year and the focal spots were carefully watched by a number of epidemiological institutions, including special plague institutes in Irkutsk, Chita, Rostov and Saratov. Whenever a case was reported, flying squads were sent to the threatened area with vaccine. They always succeeded in preventing the development of an epidemic. Soviet authorities now claim that the danger of plague has been completely eliminated.
Much more serious than plague, however, was cholera. Cholera has had a particularly bad record in Russia. It made its appearance in fifty five of the one hundred years between 1823 and 1922, and it has been estimated that during that time five and a half million people suffered from it and 2.2 million succumbed to the disease. In 1915, there was an outbreak of more than 30,000 cases of cholera at the front and in the interior of the country. A new epidemic broke out in April 1918 in Astrakhan and Saratov. It did not follow water routes, as had been customary, but followed railroad lines. It reached its climax in July and August of that year after invading 30 provinces. The epidemic was mild in character and decreased during the winter. There was another attack in 1920 from a focus in Rostov. This epidemic reached its peak in July 1921 in the lower Volga region. The figures for the years from 1918 to 1922 are the following:
Cases of Cholera
1918 41,289
1919 4,259
1920 25,923
1921 204,228
1922 86,178
The epidemiological measures applied consisted mostly of vaccination. In 1922 ten million people, including the entire Red Army, were vaccinated. The sources of water supply and the sewage systems were controlled and cleaned as much as was possible at the time. Between 1923 and 1926 a few isolated cases were observed, but after 1927 cholera completely disappeared.
This is not the case with typhoid fever and dysentery. Both diseases were endemic in tsarist Russia as a result of inadequate water supplies and inefficient control of foodstuffs. The average typhoid morbidity before 1914 was about 25 for every 10,000 inhabitants, and the rate for dysentery was somewhat higher. During the Civil War, sanitary conditions so deteriorated that morbidity from both diseases doubled. Pre-war conditions were reached in 1922, and since that time there has been a slow decrease in the incidence of both diseases. From 1923 to 1932 the morbidity amounted to from 7 to 12 cases per 10,000 persons for typhoid, and from IO to 25 for dysentery. Anti-typhoid vaccination is now used extensively, and it is compulsory for Red Army recruits and for all groups of workers, such as those living in camps, who are in particular danger. In 1940, about one m every ten civilians in the RSFSR, the Ukraine and Byelorussia was vaccinated. By 1941, the morbidity was less than one-fifth of what it had been prior to World War I, but the disease is still a cause for concern.The same is true for dysentery, particularly in the southern and eastern sections of the country.
Vaccines have been used with varying success, and much effort is now being concentrated on developing one which will be wholly satisfactory. As I have already pointed out, the Soviet government has built many new water and sewage systems, and through sanitary inspection strictly controls food products. Thus it is fighting these diseases in the most desirable way, but it will still be some time before the sanitary conditions are satisfactory everywhere.
Smallpox is a preventable disease which can be controlled through vaccination. Tsarist Russia had no law making vaccination compulsory, but the Zemstvo authorities endeavored to immunize the population and carried on regular vaccination campaigns. It was impossible, however, to reach all the people and the morbidity was very high. From 1890 to 1913 it ranged from 45 to118 for every 10,000 population5.7 During World War I, Zemstvo physicians were mobilized. As a result vaccination was neglected and in 1915 a regular smallpox epidemic broke out. It decreased the following year, flared up again in 1919, and reached its climax in 1920 with more than 150,000 reported cases. In 1919 immunization was made compulsory, and by 1936 more than ro million people were being vaccinated and re-vaccinated every year. There are still regions in the Soviet Union, however, into which the vaccinator hardly penetrates. In 1929 there were slightly over 6,000 cases or 0.37 for every 10,000 population. By 1935 the rate had dropped to 0.2. A marked improvement was observed in 1936 during which the whole country had only 400 cases of smallpox. By 1939, the disease had been completely overcome. A 1939 law of the RSFSR holds parents responsible not only for having their children vaccinated during the first year of their life but also for their re-vaccination at the ages of four to five and ten to eleven years. Re-vaccination is again required between the ages of eighteen to twenty years.
The contagious diseases of childhood, diphtheria, scarlet fever, and measles, do not present any particular problems. Diphtheria increased somewhat during the Civil War but not markedly. The extension of nurseries and other institutions for the protection of infancy and childhood has been the best possible method of preventing the spread of these diseases. Diphtheria immunization has been made compulsory for children between the ages of one and eight years, and re-immunization is common. In 1931, 400,000 children were immunized, 1,200,000 in 1932, and 10,000,000 in 1940. As a result the morbidity has dropped very con siderably; it was 31.4 from 1910-1913, and in recent years has not been above 7.6 (per 10,000 population). Following years of a further downward trend, the incidence of diphtheria again became high in 1942 under the abnormal wartime conditions. Mortality increased from both diphtheria and pneumonia during this period. Although the situation was brought under control in 1943 it will probably cause concern for several more years.
That is not the case with respect to scarlet fever and measles. Not withstanding some setbacks during the evacuation period, their incidence continued to decline during the war. Mass vaccinations against scarlet fever are carried out in many cities. Use of an anti-measles serum, which began in 1924 in a limited number of cities, was made obligatory in 193 7 for all children coming in contact with measles. T he serum has not been fully satisfactory, and much research is being carried on to develop direct methods of immunization.
Unlike other European countries, Russia always had a high incidence of such diseases as rabies, anthrax and trachoma. There are still many rabid dogs, cats and wolves in the country; in the mid-1930's it was estimated that about 70,000 persons were being bitten every year. Such cases are treated with vaccine, obtained from the Pasteur Institutes, which are to be found in all sections of the country. Anthrax still occurs in cattle-breeding regions; the morbidity in 1936 was somewhat below one for every 10,000.
The incidence of trachoma in 1913 was 63.3 per 10,000, and the dis ease was a curse among many of the national minorities. The Chuvash Autonomous Republic is an example of an area that was widely infected with it. Immediately after the Revolution, four out of every five persons in some Chuvash areas were found to be affected with trachoma. In a section where the disease had incapacitated one tenth of the population, 10,000 persons were found who had been blinded by it. By 1926, the incidence of trachoma had been lowered to forty-seven per cent of the Chuvash population.5 9 During the following decade, a network of dispensaries was built for the treatment of trachoma cases and to keep the entire populatin of the affected areas under observation. By 1936, there were 2,000 medical stations 00 giving treatment for the disease; the number of oculists and hospital beds reserved for eye cases had also grown rapidly. As a result of the vigorous attack upon the disease, among the Chuvash the morbidity rate for trachoma m 1941 was 39 per cent of what it had been in 1913, while the corresponding percentages for the former Kalmyk Autonomous Republic and the Tatar Autonomous Republic on the Volga were respectively 25 and u per cent. 61 All evidence points to a complete conquest of the disease in the not distant future.
Malaria is a great epidemiological problem in the Soviet Union. Russia always had three great malaria centers: Turkestan, the Caucasus, and the lower Volga region. About three million cases occurred every year before the Revolution, when there was only one station, in Batum, to fight the disease. It was established by private initiative and supported by private means. As a result of World War I, malaria began to spread throughout Russia. Troops from infected regions carried the disease with them wherever they went and created new foci of contagion. More than two million cases were registered in 1922, and more than four mil lion in 1923. It has been estimated, however, that the actual number was at least four times as high. The disease, which had previously been localized in the sub-tropical regions, spread to the north and even into the Arctic. At the time when the epidemic was at its height, the country had not more than from eight to ten thousand kilograms of quinine available because of the blockade. Thus it was practically impossible to treat the patients.
A systematic campaign was organized to fight the disease. In 1920, a Central Institute for Tropical Diseases was created in Moscow to serve as research, training and organizational headquarters. Since then, five smaller similar institutes have been erected in the Caucasus and three in Asia. In 1923, the first All-Union Malaria Conference was called; similar meetings have been held at regular intervals. Malaria stations were built in all threatened districts; each is equipped with laboratory, dispensary, and hospital. Physicians were trained for malarial work in special post-graduate courses. The Commissariats of Agriculture and Transportation were invited to cooperate, and the population was mobilized to take an active part in the campaign. Drainage of swamps, petrolization of water sheds, examination of the population in infected areas, and distribution of quinine were carried on systematically. Nevertheless, as late as 1929, three million cases were still registered, and rt was not possible to observe marked progress in the anti-malarial program for several more years. In 1936, 32 million persons were examined, and over 4 million were treated for the disease. Over 2,866,000 hectares of water sheds infested with malaria mosquitoes were sprayed by airplanes, while land spraying and petrolization were applied on 239,000 hectares. Two hundred thousand screens and 20 million meters of mosquito netting were distributed to collective farmers. During the summer of 1936, 500 groups of doctors and senior medical students joined the fight which was being carried on by 1,800 permanent malaria stations. Fifty thousand collective farmers took part in the 011 sprinkling and in the
delivery of medicines. Next to quinine, two Soviet preparations, plazmotsid and akrykhin, were widely used with good results. During the campaign 1,500 doctors and 2,500 feldshers working in the villages received special anti-malaria training. A hundred and twenty million rubles were spent in 1936 alone. As a result, the number of cases of malaria was reduced by 30 per cent under that for 1935 and the number of deaths by 40 per cent. Government appropriations amounting to 130 million rubles were made available for the campaign of 1937. In addition, 48 million rubles were allocated out of local budgets to maintain more than 2,000 malaria stations; 35 million rubles were appropriated for the draining of swamps and similar preventive measures.***Pravda, April 25, 1937.
With the continuance of this program, incidence of the disease continued to drop from year to year. In 1940, when twenty-seven million persons were examined for the disease, there were less than one-third the number of cases registered m 1934. (Registration of all cases is compulsory.) However, malaria was a problem for the Red Army as well as in the southern evacuation areas during World War II, and will no doubt continue to require attention for some time to come. Virtually all anti-malaria institutions and swamp-draining works in the occupied areas were destroyed by the Germans and have had to be restored.
The Soviet health authorities launched their activities in a period of great emergency when serious epidemics ravaged the country. In the short period of a quarter of a century, they created a powerful network of institutions which have already helped the general medical institutions to eliminate completely, in some cases, and to reduce considerably in most other cases, the incidence of epidemic diseases. In 1941, this special network consisted of the following institutions:
Anti-epidemic stations 1,760
Disinfection stations and mobile squads 2,288
Bacteriological laboratories 1,406
Malaria stations and points 2,945
Pasteur Institutes 120
Measles stations 282
The Soviet authorities have succeeded in this anti-epidemic program where the tsarist government failed because of their determination to protect the people's health, the health of all the people. Consequently, when another period of great emergency arrived with the German invasion in 1941, which created conditions in which epidemics might otherwise have flourished again, the excellent work of the public health authorities made it possible not only to prevent the spread of disease on both the war and home fronts, but even to continue the downward trend in some of these diseases throughout the war period. Infectious diseases are still far too prevalent in the Soviet Union, and will be so for some time to come because the country is vast and the population heterogeneous. Their conquest will not be long delayed, however, if present trends continue without major disturbance.
Social diseases are those which result primarily from bad social and economic conditions. These diseases consequently affect the working class with particular severity. The Soviet government has eliminated class distinction and has abolished exploitation. It is striving to remove the causes of social diseases by raising the economic and educational standards of the whole population. Once this goal is reached, social diseases will largely disappear. But their incidence in tsarist Russia was high, and they still continue a serious problem.
One of the most prevalent social diseases in the Soviet Union, and still one of the most frequent causes of death, is tuberculosis. For the years 1913 to 1915, the mortality rate averaged 40 per 10,000 for the whole country; 65 the Moscow death rate in 1913 from all forms of the disease was 26.6 and the St. Petersburg rate 33.6 per 10000. The Russian government did nothing to fight the disease. All efforts centered in the All-Russian Tuberculosis Association, a philanthropic organization founded by socially minded physicians and liberal laymen. Its financial resources were scanty. In the whole Russian empire in 1914, there were only 43 tuberculosis dispensaries and 18 sanatoria with 308 free beds. Fewer than a thousand beds, even including the facilities of private hospitals, were available for tuberculous patients. At the beginning of World War I, the activities of the Association were considerably reduced; the organization had broken down completely by the time of the Revolution.
As soon as the Commissariat of Public Health was organized in 1918, it launched a systematic fight against tuberculosis. A special tuberculosis department was established within the Commissariat to take charge of the campaign, and a Central Tuberculosis Institute was created in Moscow to serve as general staff. The Institute has an experimental department devoted to research in the pathological anatomy and physiology, microbiology, and epidemiology of tuberculosis. It has a clinical department for the study of pulmonary tuberculosis, tuberculosis of the bones, and tuberculosis of children. In 1936, this institute controlled five sanatoria: three for children and two for adults.
The example set by the Russian republic has been followed by the other constituent republics, and central tuberculosis institutes have been organized in Kharkov, Minsk, Tiflis, Samarkand, Alma-Ata. Besides, regional institutes have been created in Moscow, Leningrad, Ivanovo, Kazan, Sverdlovsk, and other places for the purpose of supervising the attack upon tuberculosis in their respective regions (oblasts). There were thirteen of these institutes in 1941, each with its own laboratories and clinical facilities. Their task is to conduct research, devise methods for combating the disease, and aid and advise the dispensaries of their regions.
An important and urgent task has been the training of specialized personnel. Required comprehensive courses on tuberculosis are now given in all medical schools. Several universities and most post-graduate schools have special chairs devoted to the subject. All the tuberculosis institutes give post-graduate courses to physicians and graduate about 500 specialists a year. In 1936, dispensaries and sanatoria employed about 27,000 physicians, all of whom had some specialized training. In 1941 there were more than 3,100 ranking tuberculosis specialists.
The fighting unit in the campaign against tuberculosis is the dispensary, of which there are two types. About half of them are inde pendent organizations. The other half consist of dispensaries connected with health centers. Unlike those of other countries, the Soviet dispensary undertakes diagnostic, preventive, and curative work. It at tacks all forms of tuberculosis and treats patients of all ages. Some of the dispensaries are small, while others are very large, having staffs of not fewer than from IO to 25 physicians. Such large dispensaries employ a variety of specialists, including pediatricians, surgeons, and laryngologists. All of them, however, are trained m tuberculosis. There is generally one dispensary for every district of from 150,000 to
350,000 inhabitants. Moscow has 20. Rural areas have or will have a dispensary for each region, or district.
The function of a dispensary is the prevention and control of tuberculosis in its entire district. It begins its work by making a study of the social, economic, and general health conditions of the area. It establishes contacts with all the local health agencies: health departments, health centers, trade unions, factory committees, and consultation bureaus for mother and child. If housing conditions are poor or labor conditions unsatisfactory, it makes suggestions for their improvement. Its primary function, however, is the depistage, the finding of tuberculous individuals. In this task visiting nurses play an important part; they made more than one million visits in 1940. Several dispensaries have made house to house surveys. If workers in a factory are often sick and are suspected of tuberculosis, dispensary doctors come to examine them. In a locomotive factory, for example, of 440 such workers examined, 22 were found to be tuberculous, three of them with open tuberculosis. Particular attention is given to those age and vocational groups such as adolescents, students of higher schools, people working in dusty industries, or in tuberculosis institutions, who are most likely to develop the disease. Such persons are examined periodically by dispensary physicians. All efforts are made to diagnose the disease early, to remove and treat open cases, and to supervise all other patients permanently. The growth of dispensaries (exclusive of tuberculosis departments in the general medical centers) is illustrated by the following figures:
Number of Tuberculosis Dispensaries and Stations in the USSR
1914 43
1929 498
1938 803
1939 925
1940 977
1941 1,048
The dispensaries are equipped with X-ray apparatus and laboratories, and generally have their own clinical facilities.
Night sanatoria, the first of which was opened in a Moscow dispensary in 1921, and day sanatoria also have an important role to play. Patients who are able to work but require some regular treatment and care are admitted to these sanatoria. They arrive at about six o'clock in the evening after working hours, have a hot shower or bath, change their clothes, and have dinner. Afterwards they rest for an hour or two, if possible on porches; their temperature is taken, and they are examined by a physician. They spend the time from eight until ten o'clock in the club of the institution or in undergoing medical treatment. From ten in the evening until six the next mornmg they are expected to be in bed. They then have physical exercises and breakfast, and return to work. Persons on night shifts are admitted to day sanatoria in the same way. A very important function of these part-time sanatoria is the education of patients. They are taught how to live properly in order to improve their condition. In 1941 there were 211 of these day and night sanatoria with a total of 7,526 beds.
Open cases of tuberculosis are treated in special hospital wards or, when possible, in sanatoria. In 1917, Russia possessed no special hospitals for tubercular cases, but an entire network of such institutions has since been developed and is still growing. The statistics on the number of hospital beds follow:
Number of beds 1937 1938 1939 1940 1941
for children 1,628 3,271 4,053 4,147 4,500 (app.)
Total number of
beds 13,236 17,828 21,324 24,946 28,000
In 1941, on the eve of the war, there were 898 tuberculosis sanatoria in the USSR, with a total number of 72,800 beds.67 Most of these facili ties were concentrated in the many health-resorts, where about half the beds for tuberculosis cases were reserved for children. For example, more than 16,000 of these beds were given over to children with tuberculosis of the bones and joints. The tuberculosis sanatoria were a major war casualty. In 1944, the number functioning had been reduced to 285, with a total of 23,046 beds.68 Restoration is now rapidly underway. Great attention is paid to tuberculosis of childhood. It has been found that from 5 to 10 per cent of all children with a disease usually diagnosed as influenza are actually suffering from tuberculosis. All dispensaries treat tuberculosis m children and about 40 per cent have organized chil dren's departments. Special "health kindergartens," forest schools and open-air classes in the regular schools have been created for such youngsters. In 1941, special nurseries had 2,642 beds available for them. As already indicated, the hospitals and health resorts that same year had accommodations for about 40,000 children. Sanatona and health resorts still need to be increased in number, especially in view of the fact that the last war brought not only great destruction of treatment facilities but a sudden and fresh increase in the number of cases.
Special institutions, so-called luposoria, have been organized for the treatment of cutaneous tuberculosis. There were three of these in 1934: one in Moscow with 120 beds, one near Leningrad with 170 beds, and one in Sverdlovsk with 30 beds. A labor colony is attached to the Moscow institution where mutilated patients can work.
In the treatment of tuberculosis various methods are applied according to the case. Collapse therapy, pneumothorax or thoracoplastic, is used commonly. Climatotherapy is very popular and has great possibili ties of development in the Soviet Union. A method that has given good results, which was worked out in the Regional Institute in Moscow, is the so-called polyphysiotherapy: a combination of electrical vibration massage, phototherapy, and diathermy. In 1936 vaccination with BCG was compulsory in ten cities for all children exposed to infection, for children of tuberculous parents, and for those living under bad conditions. Vaccination, which was first instituted in Kharkov, has been applied in Moscow since 1926, and it has been found that the death rate is four times lower among vaccinated groups. Since 1937, more than two million infants have been vaccinated. Much research continues to im prove the vaccine, which is now used in more than 250 communities.
While the treatment of tuberculosis does not differ basically from that used in other countries, Soviet health authorities have decidedly different views concerning the social readjustment of tuberculous people. The principle is not to send the tuberculous worker "to the land" as ' is done elsewhere, but to keep him at work in the factories. It is believed that the patient can be supervised medically much more closely in fac tories than in agricultural enterprises. A decree passed in 1935 by the Commissariat of Public Health and the Trade Union Council requires directors of all enterprises to make special provision for tuberculous workers. Their working hours may be reduced and social insurance funds will make up the balance of wages. All larger factories have special dietetic dining-rooms for such persons. In 1938, factories in Moscow, Leningrad, Kharkov, Gorky and other industrial centers had special workshops, called prophylactic workshops, for these workers. In a rubber shoe factory they have their own conveyor which moves more slowly. Since all enterprises have a definite plan for amount of production, it is obvious that a large number of tuberculous workers handicaps a plant so that many managers are not enthusiastic about employing them. In a radio factory in Voronezh, the difficulty has been overcome by letting tuberculous men work as a special group outside the plant. Thus they do not handicap the enterprise, but add to its production figures. In more serious cases, invalids from tuberculosis have organized cooperatives where they perform light work under medical supervision. Tuberculous patients are kept in their customary surroundings whenever possible. If they are skilled workers, every effort is made to prevent them from dropping to the ranks of the unskilled on account of their illness.
On the eve of World War II, the Soviet tuberculosis problem seemed well on the way to a permanent solution. Considerably earlier, in fact, statistics disclose great improvement since Revolutionary days. As early as 1931, the death rate from pulmonary tuberculosis had been cut in half in the large cities, for example to 16.3 in Leningrad and to 11.6 per 10,000 Moscow. From 1926 to 1937, the number of tuberculosis cases of all types was also halved. By 1941, the mortality rate for the entire Union was down to two-fifths of the 1913 figure, or about 8 per 10,000 cases. Absenteeism from work because of the disease was a third of what it had been in 1913. The greatest drop in the disease was observed among industrial workers. Decreases in both the number of cases and mortality were significant in the national republics.
Because of the war, however, tuberculosis remains one of the most serious health problems of the Soviet Union. The mass evacuation which had to be carried on while the tide of German invasion continued to flow eastward resulted in serious overcrowding and privation in areas which were ill-prepared to receive a large and sudden influx of people. This created a serious menace to health. Another grave health problem developed in the areas temporarily occupied by the Germans because of the deliberate maltreatment of the native population, millions of whom had to subsist on a near-starvation diet in overcrowded and unsanitary quarters, if not in dugouts amid the ruins of their homes. The tuberculosis rate began to soar, and it was found necesasry early in 1943 for the Council of People's Commissars of the USSR to take emergency measures.
In accordance with one decree issued by the Council in January 1943, there had been made available for tubercular cases by October 1944, the followmg additional facilities: 13,000 hospital beds, 4,500 beds in day sanatoria and night sanatona, more than 35,000 places for children in kindergartens, nurseries and outdoor or forest schools, and accommodation for 1,600 in invalid homes . It also became necessary to open tuberculosis departments in the general hospitals and other institutions, and to supplement the services of the overworked tuberculosis specialists with those of other physicians, especially the general practitioners and the country's 18,000 pediatricians. Supplementary food rations were made available. As a result of these and many other vigor ous measures, the death rate from the disease began to drop in 1943.
The improvement was marked by 1944, when the morbidity rate dropped to about what it had been at the begmning of World War IL Soviet health authorities still express concern over the situation, however, and continue to take many prophylactic measures, such as semi annual examinations of young industrial workers. There is no doubt that several more years of medical attack and improved living conditions are necessary before tuberculosis can be completely uprooted.
Venereal diseases were very widespread in tsarist Russia. In 1913,180.37 cases per 10,000 population were registered. Registration was supposed to be compulsory, but only persons who applied for treatment were registered. Because medical facilities were scarce, many patients were never treated at all or were treated by quacks and so were not included in the official statistics. This was particularly true of gonorrhea in rural districts.
The national minorities were heavily contaminated with venereal diseases. It has been estimated that 30 per cent of the Yakut population was infected with syphilis. In rural districts and particularly in the oriental parts of the empire, syphilis was not a venereal disease. It was spread through extra-genital infection as the result of certain peculiar customs. In many of these tribes people ate from the same bowl, drank from the same cup, licked the dishes, smoked the same water pipe, kissed icons and each other, and thus spread the disease. Soldiers returning from the front after World War I contaminated the population of their home villages, mostly with gonorrhea.
(....)
The socialist state feels responsible for all its members. It attempts to give equal opportunities to all. It opens wide the door to education and guarantees a job to everyone. If an individual becomes anti-social and resorts to crime, this means that society has made a mistake, that a man through unfortunate circumstances was deprived of opportunities. It is, therefore, the duty of society to treat him as it would treat a sick person, and aid him in his social recovery. In the process of therapy, it is essential that the self-respect of the criminal should not be weakened, but rather strengthened. Article 9 of the Criminal Code reads: "Measures of social defense shall not have as their object the infliction of physical suffering or personal humiliation. The question of retaliation or punishment does not arise."
It was to be expected that improved living conditions and the de velopment of cultural facilities would lead to a significant reduction in the incidence of crime. This has actually happened. Crime reached its peak between 1930 and1931 when the kulaks opposed the Five-Year Plan. There has been steady improvement since then. From 1933 to 1935, crimes against personal property decreased by 55 per cent, murder and manslaughter by 50 per cent, and sexual offenses by 75 per cent.81 Convictions for mismanagement of state funds increased somewhat in the mid-thirties, and there was a great deal of hooliganism until society absorbed the last of the homeless waifs and vagrant children. The severe hardships and emotional upsets caused by the last war have also apparently created new problems of crime, which the authorities are now coping with and which can be expected to disappear as Soviet life returns to the customary social pattern.
Regardless of future decreases in the amount of crime, however, there will always be some psychopaths who will become criminals. Their rehabilitation will constitute a difficult task, but one for which the medical profession should assume responsibility.










